Understanding the Purpose of an ICD
An ICD is a life-saving device implanted in patients at risk of:
-
Sudden Cardiac Arrest (SCA)
-
Ventricular Tachycardia (VT)
-
Ventricular Fibrillation (VF)
-
Severe cardiomyopathy with low ejection fraction
The device continuously monitors heart rhythm and delivers:
-
A shock to terminate life-threatening arrhythmias
-
Anti-tachycardia pacing (ATP) in selected devices
-
Backup pacing (in some systems)
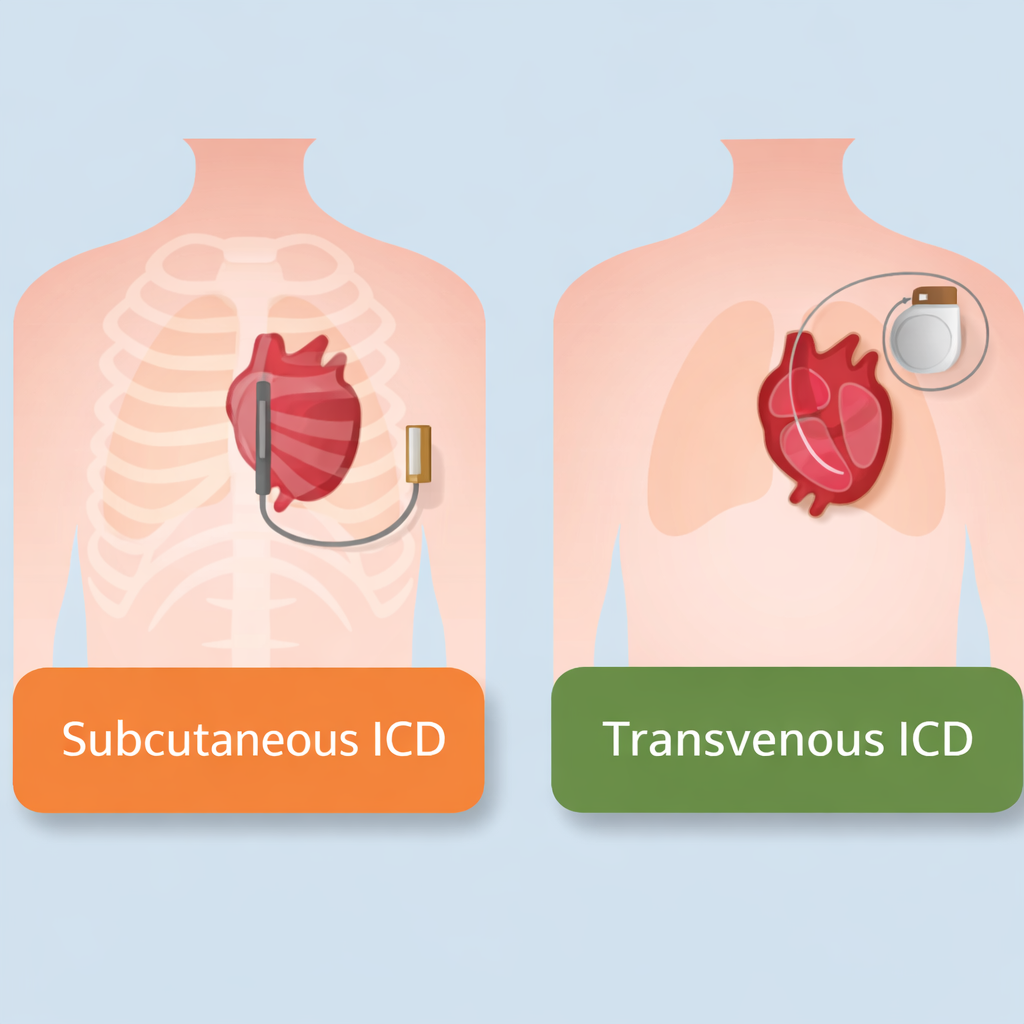
There are two main types:
-
Transvenous ICD (TV-ICD)
-
Subcutaneous ICD (S-ICD)
Let’s understand the difference.
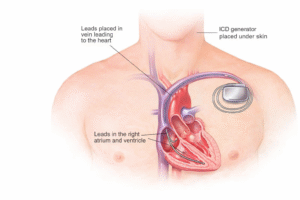
What is a Transvenous ICD (TV-ICD)?
A Transvenous ICD is the traditional and most commonly used ICD system.
How It Works
-
Leads (wires) are inserted through veins into the heart chambers.
-
The generator is implanted under the skin below the collarbone.
-
The leads sit inside the right ventricle (and sometimes right atrium).
What It Can Do
-
Deliver shocks for dangerous arrhythmias
-
Provide Anti-Tachycardia Pacing (ATP)
-
Offer bradycardia pacing if the heart rate drops
-
Act as CRT-D in heart failure (in select patients)
Advantages
-
Proven technology with decades of data
-
Can provide pacing support
-
Effective for recurrent monomorphic VT (ATP benefit)
Limitations
-
Leads inside the bloodstream
-
Risk of lead fracture over time
-
Risk of bloodstream infection
-
More complex lead extraction if infection occurs
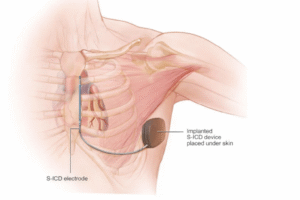
What is a Subcutaneous ICD (S-ICD)?
A Subcutaneous ICD is a newer-generation system designed to avoid placing leads inside the heart.
How It Works
-
The generator is placed on the side of the chest.
-
The lead runs just under the skin along the breastbone.
-
No wires enter the heart or bloodstream.
What It Can Do
-
Detect and terminate ventricular arrhythmias
-
Deliver defibrillation shocks
What It Cannot Do
-
Provide bradycardia pacing (long-term)
-
Provide Anti-Tachycardia Pacing (ATP)
-
Provide CRT therapy
Advantages
-
No intravascular leads
-
Lower risk of bloodstream infection
-
Ideal for younger patients needing long-term device therapy
Limitations
-
Cannot treat slow heart rhythms
-
Larger generator
-
Shock-only therapy (no ATP)
How I Make the Decision in Clinical Practice
When a patient walks into my clinic at Yashoda Hospitals, this is the structured approach I follow:
1️⃣ Does the Patient Need Pacing?
This is the most important question.
If the patient:
-
Has sinus node dysfunction
-
Has AV block
-
Needs CRT for heart failure
-
Has recurrent monomorphic VT that benefits from ATP
➡ Transvenous ICD is the better choice
If the patient:
-
Has structurally normal conduction
-
Only needs shock therapy
-
Has inherited arrhythmia syndromes (e.g., Brugada, HCM without pacing indication)
➡ Subcutaneous ICD is strongly considered
2️⃣ Age of the Patient
Younger patients (<40–50 years) are likely to live many decades with the device.
Transvenous leads:
-
May fracture over time
-
May require replacement
-
Are difficult to extract after long duration
For young patients, especially:
-
Channelopathies
-
Hypertrophic cardiomyopathy
-
Primary prevention cases
➡ I prefer S-ICD to avoid lifelong intravascular lead complications.
3️⃣ Infection Risk
Patients at high risk:
-
Diabetes
-
Kidney failure
-
Prior device infection
-
Immunocompromised state
Because S-ICD avoids bloodstream entry:
➡ It significantly reduces systemic infection risk.
In such cases, S-ICD becomes very attractive.
4️⃣ Type of Arrhythmia
Patients with:
-
Recurrent monomorphic VT
-
VT amenable to ATP termination
TV-ICD is better because ATP can terminate VT painlessly without delivering shocks.
S-ICD cannot provide ATP.
So if frequent VT is expected:
➡ Transvenous ICD is preferred.
5️⃣ Structural Heart Disease and Heart Failure
If the patient:
-
Has LVEF <35%
-
Requires Cardiac Resynchronization Therapy (CRT-D)
-
Has conduction delay (LBBB)
Only transvenous systems can provide CRT.
➡ S-ICD is not suitable.
6️⃣ Lifestyle and Body Habitus
Athletes, young active individuals:
-
May benefit from S-ICD due to less risk of lead damage inside the heart.
-
Avoid central venous obstruction.
Very thin patients:
-
May feel S-ICD generator more prominently.
Cosmetic and comfort considerations also matter.
Real-World Case Scenarios
Case 1: 32-Year-Old with Hypertrophic Cardiomyopathy
-
No pacing need
-
Primary prevention
-
Structurally preserved conduction
✅ I recommend S-ICD
Case 2: 68-Year-Old with Ischemic Cardiomyopathy
-
EF 28%
-
LBBB
-
Heart failure symptoms
✅ Needs CRT-D (Transvenous system)
Case 3: 55-Year-Old with Recurrent Monomorphic VT
-
VT terminated with ATP during EP study
✅ Transvenous ICD preferred
Case 4: 40-Year-Old with Previous Device Infection
-
Requires re-implantation
✅ S-ICD safer option
Long-Term Considerations
| Factor | Transvenous ICD | Subcutaneous ICD |
|---|---|---|
| Lead inside heart | Yes | No |
| ATP capability | Yes | No |
| Brady pacing | Yes | No |
| CRT option | Yes | No |
| Infection risk | Higher | Lower |
| Ideal for young | Moderate | Excellent |
What I Tell My Patients
I always explain:
“We are not choosing just a device. We are choosing a long-term strategy for your heart rhythm safety.”
The best ICD is the one that:
-
Protects you effectively
-
Matches your rhythm needs
-
Minimizes long-term complications
-
Aligns with your lifestyle
There is no “better” device universally. There is only the right device for the right patient.
Frequently Asked Questions (FAQs)
1. Is S-ICD safer than Transvenous ICD?
S-ICD reduces bloodstream infection risk but cannot provide pacing. Safety depends on patient profile.
2. Does S-ICD give more painful shocks?
Shock energy is slightly higher, but patients generally do not feel difference as shocks are delivered during arrhythmia.
3. Can S-ICD be converted to Transvenous ICD later?
Yes, if pacing becomes necessary in future.
4. How long do ICD batteries last?
Typically:
-
5–10 years depending on usage
-
Frequent shocks reduce battery life
5. Can I exercise with an ICD?
Yes. Most patients resume normal activity after recovery. Contact sports may require precautions.
6. Will airport security affect my ICD?
No major risk, but always carry your ICD identification card.
7. Is the procedure major surgery?
No. It is a minimally invasive procedure performed under local anesthesia with sedation.
8. How long is hospital stay?
Usually 1–3 days depending on patient condition.
Final Thoughts
Choosing between Subcutaneous and Transvenous ICD is a thoughtful, patient-centered decision.
As technology advances, we now have safer and more customized options. The key is individualized risk assessment and shared decision-making.
If you or your family member has been advised ICD implantation, understanding these differences can help you make a confident, informed decision.
Doctor Details
Dr. M.S. Chandramouli
MD, DM, IDCCM, PDF(EP), ECDS
Consultant Electrophysiologist and Heart Failure Specialist
Yashoda Hospitals
Consultation Location:
Alexander Rd, Kummari Guda, Shivaji Nagar, Secunderabad, Telangana 500003
Phone: 906 342 0686
Hours: Open 24 hours
For expert evaluation of heart rhythm disorders, ICD implantation, VT ablation, and advanced electrophysiology care, schedule a consultation.