Atrial fibrillation (AF) is one of the most common rhythm disorders seen in cardiology practice. For patients whose symptoms continue despite medicines, pulmonary vein isolation (PVI) can play an important role in restoring rhythm control. This blog explains AF in simple language and walks readers through a real-world cryoablation-based PVI case shown in the uploaded presentation.
What is atrial fibrillation?
Atrial fibrillation is an arrhythmia in which the upper chambers of the heart, called the atria, stop beating in an organized way and instead activate rapidly and chaotically. In practical terms, that means the heart’s normal electrical rhythm is disturbed, and the pulse may become fast, irregular, or both. Some people feel this immediately as palpitations or a fluttering sensation, while others notice only tiredness, reduced stamina, breathlessness, or unexplained anxiety-like episodes. AF can occur in short bursts, known as paroxysmal AF, or it can continue for longer periods as persistent AF.
The uploaded presentation introduces AF as a disorder characterized by chaotic electrical activity and highlights common symptoms such as palpitations, fatigue, and anxiety. That makes it a useful starting point for patient education, because many people do not realize that what feels like stress, weakness, or sudden uneasiness may actually be a rhythm problem. In clinical practice, an ECG remains the key first step in confirming the diagnosis and understanding the rhythm pattern.
Why does AF matter? Because the heart does not pump as efficiently when the atria are not contracting in a coordinated way. Over time, AF can affect quality of life, exercise tolerance, and symptom burden. For some patients, medication is enough to control the rate or rhythm. For others, especially those with recurrent symptomatic episodes, an electrophysiology-based procedure may be recommended to target the source of the abnormal electrical triggers.
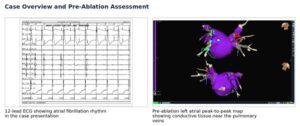
Figure 1. Case overview from the uploaded presentation: the documented AF rhythm on ECG and the pre-ablation left atrial map.
A case snapshot from the presentation
The case described in the presentation is that of a 70-year-old woman who experienced repeated episodes of anxiety with random onset. A 12-lead ECG demonstrated atrial fibrillation rhythm, and an electrophysiology study with cryoablation was recommended. This kind of case summary is valuable for a website blog because it brings the topic out of theory and into a real patient journey: symptoms, diagnosis, evaluation, intervention, and confirmation of success.
Not every patient with AF needs ablation, and not every episode of palpitations means AF. But when symptoms are persistent, recurrent, or difficult to control, electrophysiology evaluation helps determine whether the patient is a good candidate for an interventional rhythm-control strategy. The decision is individualized and depends on symptom burden, type of AF, associated heart disease, medication response, and overall clinical context.
What is pulmonary vein isolation (PVI)?
Pulmonary vein isolation is one of the most widely used catheter ablation strategies for treating atrial fibrillation. The reason it is so important lies in where AF often begins. In many patients, the triggers that start atrial fibrillation arise near the openings, or ostia, of the pulmonary veins where they connect to the left atrium. When these trigger zones fire abnormally, they can repeatedly disturb the heart’s rhythm.
The goal of PVI is therefore not to remove anything from the heart, but to electrically isolate these trigger regions from the rest of the left atrium. In simple language, the operator creates a controlled ring of scar around the pulmonary vein openings so the abnormal impulses can no longer spread into the atrium and sustain AF. The presentation explains this concept clearly by describing the creation of ablation lesions at the pulmonary vein ostia to ‘silence’ the ectopic foci.
In this case, cryoablation was used. Cryoablation works by applying very low temperatures to the target tissue through a catheter-based system. Rather than using heat, it uses cold energy to create the lesion. The purpose is the same: interrupt the faulty electrical pathway while protecting the surrounding anatomy through careful imaging, positioning, and monitoring.
Understanding the pre-ablation map
One of the most informative images in the presentation is the pre-ablation left atrial peak-to-peak potential map. This map shows where electrical activity is being conducted before treatment. The highlighted conduction near the pulmonary veins helps explain why those areas become the procedural focus. For patients and families, these images can be especially powerful because they convert an invisible electrical problem into something visual and understandable.
Website readers may not need every technical detail, but they do benefit from the larger message: ablation is not guesswork. Modern electrophysiology procedures are guided by mapping, signal interpretation, and imaging. That is what allows the operator to move from diagnosis to precise treatment in a structured, reproducible way.
Step-by-step: how this cryoablation procedure progressed
The presentation walks through each stage of pulmonary vein isolation, showing both fluoroscopic and signal-based confirmation. This is ideal material for a detailed website article because it helps readers appreciate that successful AF ablation is a sequence of verified steps rather than a single instant event.
Step 1 involved isolation of the left inferior pulmonary vein (LIPV). The fluoroscopic view showed catheter positioning, and the follow-up signals demonstrated that no residual potentials were noted in the LIPV area after ablation. In practical terms, that means the electrical activity from that vein had been successfully silenced.
Step 2 focused on the left superior pulmonary vein (LSPV). The presentation includes both pre-ablation and post-ablation signal tracings. This comparison is important because it visually demonstrates the difference before and after treatment. Before ablation, measurable signals are still seen. After ablation, those signals are suppressed, supporting successful isolation.
Step 3 then moved to the right superior pulmonary vein (RSPV), again using a combination of fluoroscopic guidance and mapping views. Step 4 addressed the remaining vein, completing the full four-vein strategy. This staged progression reflects the core principle of a thorough PVI: each pulmonary vein must be assessed and confirmed, not simply assumed to be isolated.
From a patient-education perspective, one of the best ways to explain this is to say that the procedure treats the main doorways through which AF triggers commonly enter the atrium. By sealing off each of those doorways electrically, the procedure aims to reduce or eliminate the abnormal rhythm episodes that were causing symptoms.
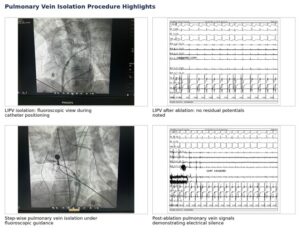
Figure 2. Selected procedural images from the presentation showing step-wise pulmonary vein isolation and post-ablation signal changes.
What the post-ablation findings tell us
At the end of the presentation, the post-ablation left atrial map shows that the four pulmonary vein branches no longer exhibit significant potentials. The concluding slide summarizes the outcome in three clinically meaningful points: the pulmonary veins were completely silenced, there was no damage to surrounding cardiac structures, and atrial fibrillation was non-inducible at the end of the procedure.
These are more than technical remarks. Together, they capture the three goals of a successful intervention: effectiveness, safety, and procedural confirmation. Effectiveness means the abnormal pathways were isolated. Safety means the treatment was delivered without evident injury to nearby structures. Confirmation means the electrophysiology findings at the end of the case supported the intended endpoint.

Figure 3. Post-ablation assessment from the uploaded presentation demonstrating electrical silence after pulmonary vein isolation.
Who may benefit from PVI?
Pulmonary vein isolation is generally considered in patients with symptomatic atrial fibrillation when medication alone is not giving adequate control, is not tolerated well, or is not the preferred long-term strategy. It is especially relevant in patients whose quality of life is affected by recurrent episodes of palpitations, fatigue, breathlessness, reduced exertional capacity, or distressing rhythm-related symptoms.
That said, PVI is not a one-size-fits-all treatment. Careful evaluation is essential. Doctors consider the pattern of AF, the size and function of the heart, associated illnesses, risk of stroke, medication history, and the patient’s treatment goals. A good website article should make this point clearly: ablation is a highly specialized treatment, and candidacy should always be decided after expert consultation with a cardiologist or electrophysiologist.
Recovery, expectations, and follow-up
Another important patient message is that ablation is part of rhythm management, not a substitute for comprehensive heart care. Even after a successful procedure, follow-up remains important. Some patients may continue medicines for a period of time. Others may need rhythm monitoring, repeat ECGs, or longer-term decisions on anticoagulation depending on their overall stroke risk profile. Symptom improvement may be dramatic, but long-term success still depends on regular review and appropriate lifestyle and risk-factor management.
In website communication, this section is where trust is built. Readers should come away informed, not overpromised. A strong and balanced message would be: PVI can offer meaningful symptom relief and rhythm control for the right patient, but outcomes depend on individual disease characteristics, procedural planning, and follow-up care.
Why this case matters for patient awareness
The strength of the uploaded presentation lies in how clearly it shows the logic of treatment. First, AF is identified on ECG. Second, the anatomy and electrical behavior of the left atrium are mapped. Third, each pulmonary vein is isolated in sequence. Finally, the endpoint is confirmed with post-ablation signals and maps. That structure makes the material ideal for a website blog focused on awareness, because it answers the key patient questions: What is the problem? Why was this treatment chosen? What exactly was done? How do doctors know it worked?
For hospitals and specialists, publishing such a blog can also help demystify electrophysiology procedures. Many patients hear the words ‘ablation’ or ‘catheter procedure’ and imagine something far more frightening or vague than what actually happens. Explaining the process through a real case, supported by images, makes advanced arrhythmia care feel more understandable and more approachable.
Conclusion
Atrial fibrillation can be physically exhausting and emotionally unsettling, especially when episodes happen unpredictably. Pulmonary vein isolation offers a focused way to treat one of the most common mechanisms behind AF by targeting the abnormal triggers near the pulmonary veins. In the case presented by Dr. Chandra Mouli at Yashoda Secunderabad, cryoablation was used to isolate all four pulmonary veins, and the post-procedure findings showed complete electrical silence with AF rendered non-inducible.
For a website audience, the key takeaway is simple: AF is treatable, and modern electrophysiology gives specialists tools to diagnose the rhythm problem precisely and treat it in a targeted way. Patients with recurrent symptoms should not ignore palpitations, fatigue, or unexplained rhythm-related discomfort. Timely assessment can open the door to effective treatment strategies tailored to the individual patient.
Disclaimer
This article is for educational purposes only and should not be treated as a substitute for medical advice, diagnosis, or treatment. Treatment decisions for atrial fibrillation, including the need for catheter ablation or pulmonary vein isolation, must be made only after evaluation by a qualified cardiologist or electrophysiologist.
Frequently Asked Questions
What is atrial fibrillation?
Atrial fibrillation, or AF, is a heart rhythm disorder in which the upper chambers of the heart beat in a fast and disorganized way. It can cause palpitations, fatigue, breathlessness, weakness, or anxiety-like episodes.
What is pulmonary vein isolation?
Pulmonary vein isolation is a catheter ablation procedure used to treat atrial fibrillation. It works by electrically isolating the abnormal trigger areas near the pulmonary veins so they cannot continue to disturb the heart rhythm.
Is pulmonary vein isolation the same as open-heart surgery?
No. PVI is a minimally invasive catheter-based electrophysiology procedure. It is usually performed through blood vessels using specialized catheters, mapping, and imaging guidance.
Who may need PVI for atrial fibrillation?
PVI may be considered for patients with symptomatic atrial fibrillation when medicines are not giving adequate control, are not tolerated well, or when a rhythm-control strategy is preferred after specialist evaluation.
How do doctors know whether the procedure worked?
During the procedure, doctors confirm electrical isolation of the pulmonary veins using signal recordings, mapping, and endpoint testing. In the uploaded case, the post-ablation findings showed complete electrical silence and AF was non-inducible at the end of the procedure.
Can AF come back after ablation?
Some patients get long-term relief after ablation, while others may still need medicines, monitoring, or additional treatment depending on the type of AF, heart condition, and overall risk profile.
Is follow-up still important after ablation?
Yes. Follow-up is essential after PVI. Patients may need ECGs, rhythm monitoring, medication review, and ongoing decisions related to stroke prevention and long-term heart health.
When should someone see a heart rhythm specialist?
Anyone with repeated palpitations, unexplained fatigue, breathlessness, dizziness, or episodes of irregular heartbeat should seek medical evaluation. Timely assessment helps determine whether the symptoms are due to AF or another rhythm disorder.
Suggested website disclaimer
This article is for educational purposes only and should not be treated as a substitute for medical advice, diagnosis, or treatment. Treatment decisions for atrial fibrillation, including the need for catheter ablation or pulmonary vein isolation, must be made only after evaluation by a qualified cardiologist or electrophysiologist.
Reference note for web team
Primary case images and procedural sequence in this blog were adapted from the uploaded presentation titled ‘Pulmonary Vein Isolation: Atrial Fibrillation’ by Dr. Chandra Mouli, Yashoda Secunderabad. General explanatory framing aligns with standard patient-information concepts used by major cardiology organizations and hospitals.
Doctor Details
About the Doctor
Dr. M. S. Chandramouli
Senior Consultant Electrophysiologist
Qualifications:
MBBS, MD (General Medicine), DM (Cardiology)
Specialization:
Clinical Cardiology & Cardiac Electrophysiology
Expertise:
-
Atrial Fibrillation Management
-
Catheter Ablation for Heart Rhythm Disorders
-
Pulmonary Vein Isolation (PVI)
-
Complex Arrhythmia Ablation
-
Pacemaker & ICD Implantation
-
Cardiac Resynchronization Therapy (CRT)
Hospital:
Yashoda Hospitals, Secunderabad